Cervical Disc Replacement
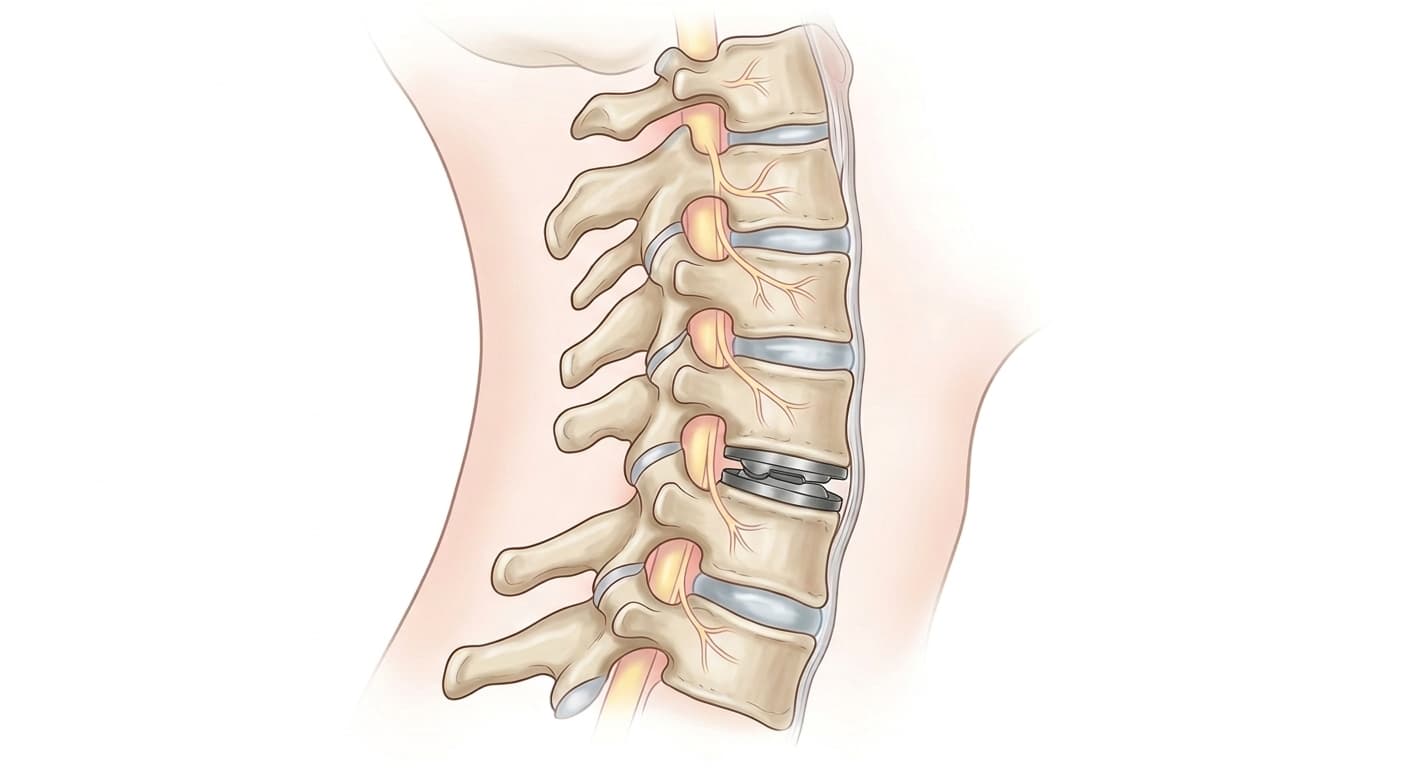
Cervical disc replacement (cervical arthroplasty) removes a damaged disc in the neck and replaces it with an artificial disc implant that allows continued motion at that spinal level. It is an alternative to anterior cervical discectomy and fusion (ACDF) for selected patients. The procedure is performed through a small incision at the front of the neck. Multiple randomized trials have shown disc replacement preserves motion and produces equivalent or better outcomes than fusion at 7-10 year follow-up, with lower rates of adjacent-level disease.
Find a SurgeonWhat is Cervical Disc Replacement?
Cervical disc replacement (cervical arthroplasty) removes a damaged disc in the neck and replaces it with an artificial disc implant that allows continued motion at that spinal level. It is an alternative to anterior cervical discectomy and fusion (ACDF) for selected patients. The procedure is performed through a small incision at the front of the neck. Multiple randomized trials have shown disc replacement preserves motion and produces equivalent or better outcomes than fusion at 7-10 year follow-up, with lower rates of adjacent-level disease.
Typical cost: $25,000 - $50,000. Cervical disc replacement is FDA-approved and covered by most major insurers and Medicare when diagnostic criteria are met. Coverage decisions often hinge on documented conservative treatment failure and imaging that correlates with clinical symptoms.
Last reviewed June 15, 2026 by AdvOrtho Editorial Team
Informational, not medical advice
Who Needs Cervical Disc Replacement?
Patients with a herniated disc or degenerative disc in the cervical spine causing arm pain (radiculopathy), numbness, or weakness that has not improved after 6-12 weeks of conservative treatment: physical therapy, anti-inflammatory medications, and cervical epidural steroid injections. Candidates must have adequate bone quality and no significant arthritis in the small joints behind the disc (facet joints). Disc replacement is typically offered for one or two adjacent levels; fusion remains the standard for three or more levels.
What to Expect
Recovery Timeline
Mild to moderate neck soreness at the incision site. Swallowing may be slightly uncomfortable for 1-2 days. Most patients return home the same day or next morning.
Return to light sedentary work for many patients. Avoid heavy lifting and twisting. Post-operative X-rays confirm implant position.
Physical therapy begins. Most arm pain from the nerve resolves within this window, though some nerve numbness can linger longer.
Return to desk work and light activity. Cervical range of motion exercises. No high-impact activity.
Full return to most activities for most patients. Follow-up imaging at 6 months to assess implant position and motion.
Risks & Complications
- Dysphagia (difficulty swallowing) in the first few weeks
- Hoarseness from retraction of the recurrent laryngeal nerve (usually temporary)
- Implant migration requiring revision surgery
- Adjacent-level disc degeneration (lower rate than after fusion, but still occurs)
- Infection
- Nerve or spinal cord injury (rare with experienced surgeons)
- Need for conversion to fusion if the replacement fails
Frequently Asked Questions
What is the difference between cervical disc replacement and ACDF?
Both procedures remove the damaged disc through the front of the neck. ACDF (fusion) fills the empty space with a bone graft and plates the adjacent vertebrae together so they grow into one solid segment. Disc replacement puts in an artificial disc that continues to move. The practical difference is range of motion: fusion eliminates motion at that level, which increases stress on the discs above and below over time. Disc replacement preserves motion and appears to reduce that adjacent-level stress, though long-term data beyond 10 years is still accumulating.
Am I too old for cervical disc replacement?
Age alone is not a disqualifying factor. The more relevant issue is bone quality and the degree of facet joint arthritis behind the disc. If there is significant arthritis in the facet joints, the replaced disc can't move properly and fusion is usually the better choice. Many patients in their 50s and 60s remain good candidates; your surgeon will evaluate CT imaging of the facet joints to determine which procedure fits your anatomy.
How long do artificial disc implants last?
Cervical disc replacements have been in use since the early 2000s. Ten-year data from randomized trials shows good implant survival with low rates of reoperation (roughly 4-5%). Longer-term data continues to accumulate, but the polyethylene and metal components appear durable. The bigger concern at longer follow-up is adjacent-level disease in the discs next to the implant, though this rate appears lower than after fusion.
Find a surgeon for Cervical Disc Replacement
Compare orthopedic surgeons who perform this procedure.
Search surgeonsEstimated Cost
$25,000 - $50,000. Cervical disc replacement is FDA-approved and covered by most major insurers and Medicare when diagnostic criteria are met. Coverage decisions often hinge on documented conservative treatment failure and imaging that correlates with clinical symptoms.
Related Specialty
Spine Specialists →Related Conditions
Other Procedures
From the Resource Center
This information is for educational purposes only. Costs are estimates and vary by location, surgeon, and insurance. Always consult a qualified healthcare provider.