Developmental Dysplasia of the Hip, or DDH, is a condition that sounds intimidating, but for parents, understanding it early can make all the difference. When your baby is born, you imagine a perfect little human, and hearing about a potential issue with their hips can be unsettling. However, DDH is relatively common, affecting about 1 in 1,000 live births, and the good news is that with early detection and proper treatment, the vast majority of babies go on to live completely normal, active lives. DDH isn’t just a single problem, though; it’s a spectrum of conditions where the ball at the top of the thigh bone (femoral head) doesn't fit correctly into the hip socket (acetabulum).
What Exactly Is DDH? It's More Than Just a "Dislocated Hip"
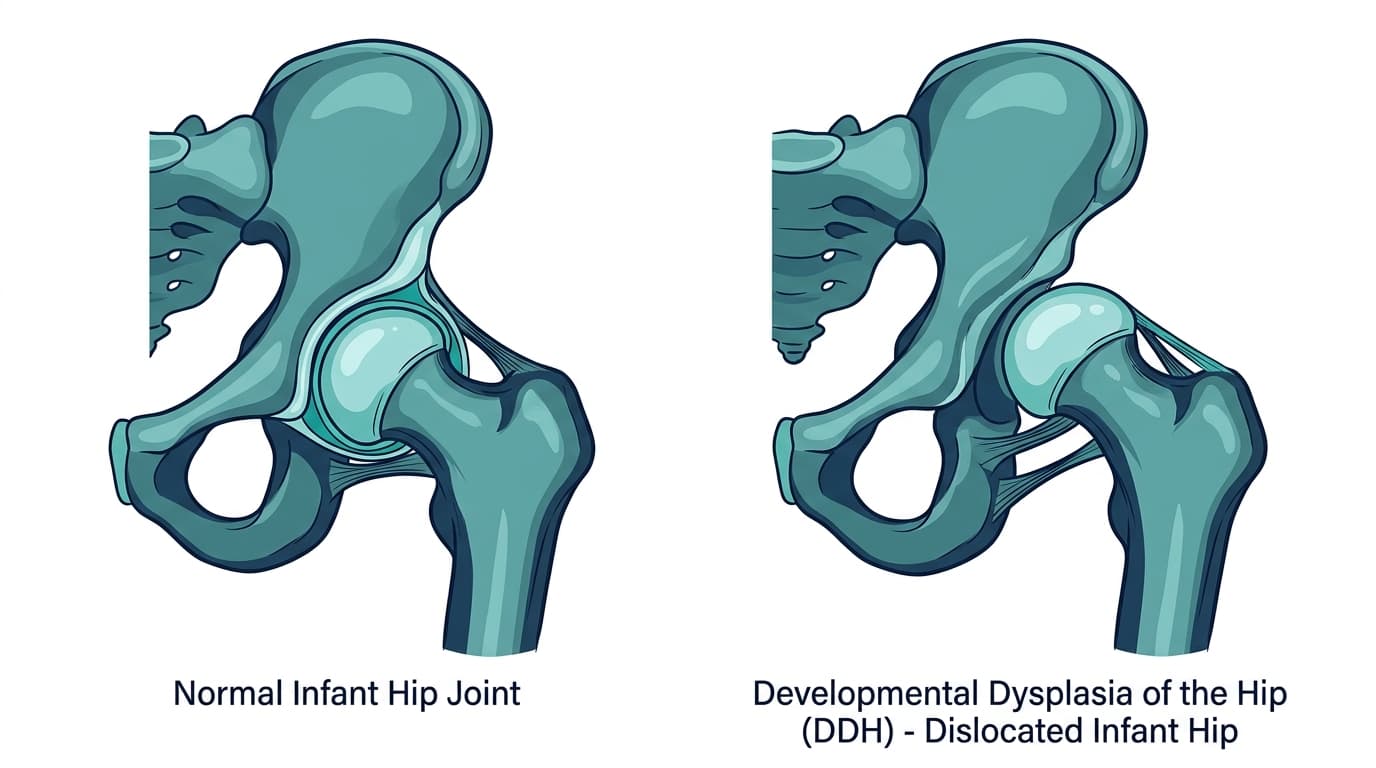
Think of your hip joint like a ball and socket. The femoral head is the ball, and the acetabulum is the socket. In a healthy hip, the ball sits snugly and securely within the socket, allowing for smooth, unrestricted movement. With DDH, this relationship isn't quite right.
The term "dysplasia" means abnormal development. So, DDH describes a hip joint that has developed, or is developing, abnormally. It’s not always a fully dislocated hip from day one. It can range from a hip that is simply "loose" or unstable, meaning the ball can easily move out of the socket but pops back in, to a hip where the ball is partially out of the socket (subluxated), or even a hip where the ball is completely out of the socket and sitting somewhere else (dislocated).
This condition isn't necessarily present at birth; it can develop over the first few months or even years of life, which is why ongoing monitoring is so important. The hip joint is primarily cartilage in newborns, which means it’s soft and moldable. If the femoral head isn’t sitting correctly in the acetabulum, the socket won’t develop its proper deep, cup-like shape, leading to a shallow socket that can't hold the ball securely. This is the core issue we’re trying to prevent and correct.
Who's At Risk? Understanding the Odds
While any baby can develop DDH, certain factors increase the likelihood. Knowing these risk factors doesn't mean your baby will have DDH, but it does mean your pediatrician or pediatric orthopedic surgeon might recommend additional screening.
One of the strongest risk factors is being a firstborn girl. Girls are about four to five times more likely to develop DDH than boys. Why firstborn? It's thought that the uterus is tighter in first pregnancies, restricting fetal movement.
Breech presentation, especially frank breech (where the baby's bottom is down and legs are straight up by the head), significantly elevates the risk. Babies born in the breech position have a 10-20% chance of having DDH, compared to about 1% for babies in a head-down position. The way the legs are held straight and together in the womb during breech presentation can prevent the natural hip flexion and abduction that encourages proper socket development. If your baby was breech, even if their initial exam seems normal, an ultrasound is typically recommended.
A family history of DDH also plays a role. If a parent or sibling had DDH, your baby's risk increases by about 10-20%. It’s not a simple genetic inheritance pattern, but there's definitely a familial predisposition. Other less common risk factors include oligohydramnios (low amniotic fluid) and associated conditions like torticollis (wry neck) or metatarsus adductus (a foot deformity). These conditions suggest a restricted environment in the womb, which can impact hip development.
Catching DDH Early: The Importance of Screening
Early detection is the absolute cornerstone of successful DDH treatment. The earlier we catch it, the simpler and more effective the interventions tend to be. This is why hip exams are standard practice for newborns and infants.
When your baby is first born, the pediatrician or obstetrician will perform specific hip maneuvers called the Barlow and Ortolani tests. These are gentle examinations designed to check for hip stability. The Barlow test attempts to gently dislocate an unstable hip, while the Ortolani test attempts to gently relocate an already dislocated hip. These tests are performed by flexing the baby's hips and knees, then gently moving the legs in specific ways while feeling for a "clunk" or "click" that indicates movement of the femoral head in and out of the socket. Don't worry, these tests don't hurt your baby, and they are quick.
These clinical exams are excellent in the newborn period, but they become less reliable after 2-3 months of age because the hip joint naturally stiffens, making it harder to elicit those tell-tale clicks. This is where imaging comes in.
For high-risk infants (like those born breech, with a family history of DDH, or with an abnormal clinical exam), an ultrasound of the hips is typically recommended around 4-6 weeks of age. Ultrasound is fantastic because it allows us to visualize the hip joint before the bones have fully ossified (hardened). We can see the cartilage, which makes up most of the newborn hip, and measure the depth and angle of the socket. It's painless, involves no radiation, and provides a clear picture of the hip's anatomy and stability.
After about 4-6 months of age, the bones in the hip begin to ossify more significantly. At this point, ultrasound becomes less useful because it can't penetrate bone well. If concerns persist or are newly identified, an X-ray becomes the diagnostic tool of choice. X-rays show the bony structures and allow us to assess the relationship between the femoral head and the acetabulum, as well as the development of the socket. This transition from ultrasound to X-ray is a natural part of infant development and imaging protocols.
The Pavlik Harness: Your First Line of Defense
If DDH is diagnosed in the first few months of life, the Pavlik harness is usually the first line of treatment. It's remarkably effective and, frankly, quite ingenious in its simplicity. The Pavlik harness is a soft, cloth harness with straps that hold your baby's hips in a specific position: flexed (knees bent up towards the chest) and abducted (legs spread out like a frog). This "frog-leg" position is the magic.
How does it work? By keeping the femoral head centered deeply within the hip socket, the Pavlik harness essentially provides the optimal environment for the socket to develop properly. The pressure from the femoral head helps to deepen the acetabulum, guiding its growth into a normal, cup-like shape. It’s not a rigid cast; it allows for some movement, which is important for hip development, but it prevents the hips from extending and adducting (straightening and coming together), which are the positions that would push the femoral head out of the socket.
Your baby will typically wear the Pavlik harness for 23 hours a day. It's usually only removed for diaper changes and supervised bathing, and often only after your doctor gives the go-ahead for temporary removal. The treatment duration usually ranges from 6 to 12 weeks, depending on the severity of the DDH and how quickly the hip stabilizes and develops.
I understand this sounds like a lot. Parents often worry about how it will affect their baby's comfort, their ability to bond, or even simple tasks like dressing. But most babies tolerate the harness remarkably well. They adapt quickly, and the benefits far outweigh the temporary inconvenience. The success rates are incredibly high, around 90%, especially when treatment starts before 3 months of age. We see the best outcomes when the hip is still very moldable. Potential issues are rare but include skin irritation (which can usually be managed with proper harness care and hygiene) and, very rarely, temporary femoral nerve palsy, which resolves once the harness position is adjusted.
When the Pavlik Harness Isn't Enough: Closed Reduction and Spica Casting
Sometimes, despite our best efforts with the Pavlik harness, it doesn't work. This might happen if the DDH was diagnosed later, if the initial dislocation was very severe, or occasionally, simply because the hip doesn't respond as expected. If the Pavlik harness fails to achieve hip stability or proper development, the next step is typically a closed reduction followed by a spica cast.
A closed reduction means that a pediatric orthopedic surgeon manually puts the femoral head back into the hip socket without making an incision. This procedure is performed under general anesthesia, so your baby will be asleep and comfortable. Once the hip is successfully reduced, a spica cast is applied.
A spica cast is a rigid cast that covers the baby's torso from the chest or waist down to the ankles, often with a bar connecting the legs to maintain the proper frog-leg position. This cast is a much more restrictive measure than the Pavlik harness, designed to keep the hip perfectly still and stable while it heals and the socket develops. Your baby will typically wear the spica cast for about 12 weeks, though this can vary. Sometimes, cast changes are needed during this period to accommodate growth or if the cast becomes soiled.
Life with a spica cast presents new challenges for parents. Hygiene, especially diapering, requires careful technique. Dressing your baby will involve specialized clothing designed to fit over the cast. Mobility will be limited, and transportation, especially in car seats, will need special adaptations. This is a tough period, no doubt, but it's a critical step to achieve a stable, healthy hip. We know it's a big ask, but it's often the necessary step to avoid more invasive procedures down the road.
Open Surgery: A Last Resort for Stubborn Hips
In some situations, particularly if closed reduction isn't successful or if DDH is diagnosed much later (for example, after 18-24 months of age), open surgery becomes necessary. This is a more involved procedure where the surgeon makes an incision to directly visualize the hip joint.
During open surgery, the surgeon might need to clear any tissue that is blocking the femoral head from seating properly in the socket. They will then place the femoral head back into the acetabulum. In older children, or when the hip socket is very shallow, the surgeon might also perform an osteotomy. This involves cutting and reshaping the bones of the pelvis or femur to create a deeper, more stable socket and improve the alignment of the hip joint.
Open surgery is a major undertaking, and the recovery is longer and more complex than with a Pavlik harness or even a closed reduction. After surgery, your child will typically be placed in a spica cast for several weeks or months to allow the bones and tissues to heal. Physical therapy will usually follow the cast removal to help regain strength and range of motion. The goal, always, is to create a stable, well-covered hip joint that will function well throughout life.
The Long Game: What Happens If DDH Goes Untreated?
The reason we put so much effort into early detection and treatment of DDH is because the consequences of untreated DDH can be significant and life-altering. If the hip remains unstable or dislocated, the shallow socket will never develop properly.
In older children, untreated DDH often leads to a noticeable limp, sometimes called a Trendelenburg gait. The child might have pain, especially with activity, and a leg length discrepancy can develop, where one leg appears shorter than the other. The hip joint won't be able to function normally, leading to limited range of motion and weakness.
Perhaps the most serious long-term consequence is the early onset of osteoarthritis. Because the hip joint isn't properly aligned, the cartilage that cushions the joint wears down unevenly and prematurely. People with untreated DDH often develop severe hip pain and debilitating arthritis in their 30s or 40s, sometimes even earlier. This usually necessitates total hip replacement surgery at a relatively young age, and even then, the outcomes can be more challenging than a typical hip replacement due to the altered anatomy.
These are significant, preventable problems. This is why we advocate so strongly for diligent screening and prompt intervention.
Swaddling and Hip Health: A Critical Conversation
Let's address the swaddling controversy directly. Swaddling can be wonderful for calming a newborn, and I understand why parents love it. However, how you swaddle matters immensely for hip health.
Traditional swaddling, where a baby's legs are wrapped tightly straight down and pressed together, can actually increase the risk of DDH or worsen an existing instability. This position prevents the hips from flexing and abducting naturally, which are the very movements that encourage proper socket development. When the hips are forced into extension and adduction, it puts pressure on the femoral head to move out of the shallow socket.
The key is "hip-healthy" swaddling. This means allowing your baby's hips to flex and abduct freely, mimicking that natural "frog-leg" position. Their knees should be able to bend, and their legs should be able to splay outwards. Many swaddling products on the market are designed with this in mind, often having a wider, looser bottom portion. If you're using a blanket, make sure there's plenty of room for your baby's legs and hips to move naturally underneath the wrap. Always ensure your baby can move their hips and knees to kick and stretch, even when swaddled. This isn't just about comfort; it's about giving those developing hip joints the space they need.
The Bottom Line: Why Early Detection Is Everything
I cannot emphasize enough how important early detection is when it comes to Developmental Dysplasia of the Hip. When DDH is caught in the first few months of life, treatment is generally non-surgical, less invasive, and has incredibly high success rates. A Pavlik harness, while requiring parental commitment, is a far cry from surgery and a spica cast.
When DDH is diagnosed later, the treatments become progressively more invasive, more complex, and carry a higher risk of complications and potential for residual problems. The recovery periods are longer, the impact on family life is greater, and the long-term prognosis, while still good with appropriate treatment, is generally not as optimal as with early intervention. We want to avoid that limp, the leg length difference, and especially the early arthritis. These are almost entirely preventable with prompt, effective care.
If your pediatrician expresses any concern about your baby's hips, or if your baby has any of the risk factors we discussed (breech presentation, family history of DDH, or abnormal exam), don't hesitate to seek a consultation. If your baby was breech or has a family history of DDH and hasn't had a hip ultrasound by 6 weeks of age, you should proactively ask your pediatrician about it. Furthermore, if you ever notice signs like uneven skin folds on your baby's thighs or buttocks, one leg appearing shorter than the other, or a persistent hip click or clunk, contact a pediatric orthopedic surgeon directly. You don't necessarily need a general practitioner referral for these specific concerns. An early visit to a specialist can make all the difference in your child's long-term hip health.


