Most people who get a herniated disc diagnosis hear it and immediately picture surgery. That's almost never where this ends up. About 90% of herniated discs resolve with conservative treatment over six to twelve weeks. The surgery conversation is real, but it's reserved for a specific subset of patients - not everyone who has pain shooting down their leg.
What's Actually Happening Inside Your Spine
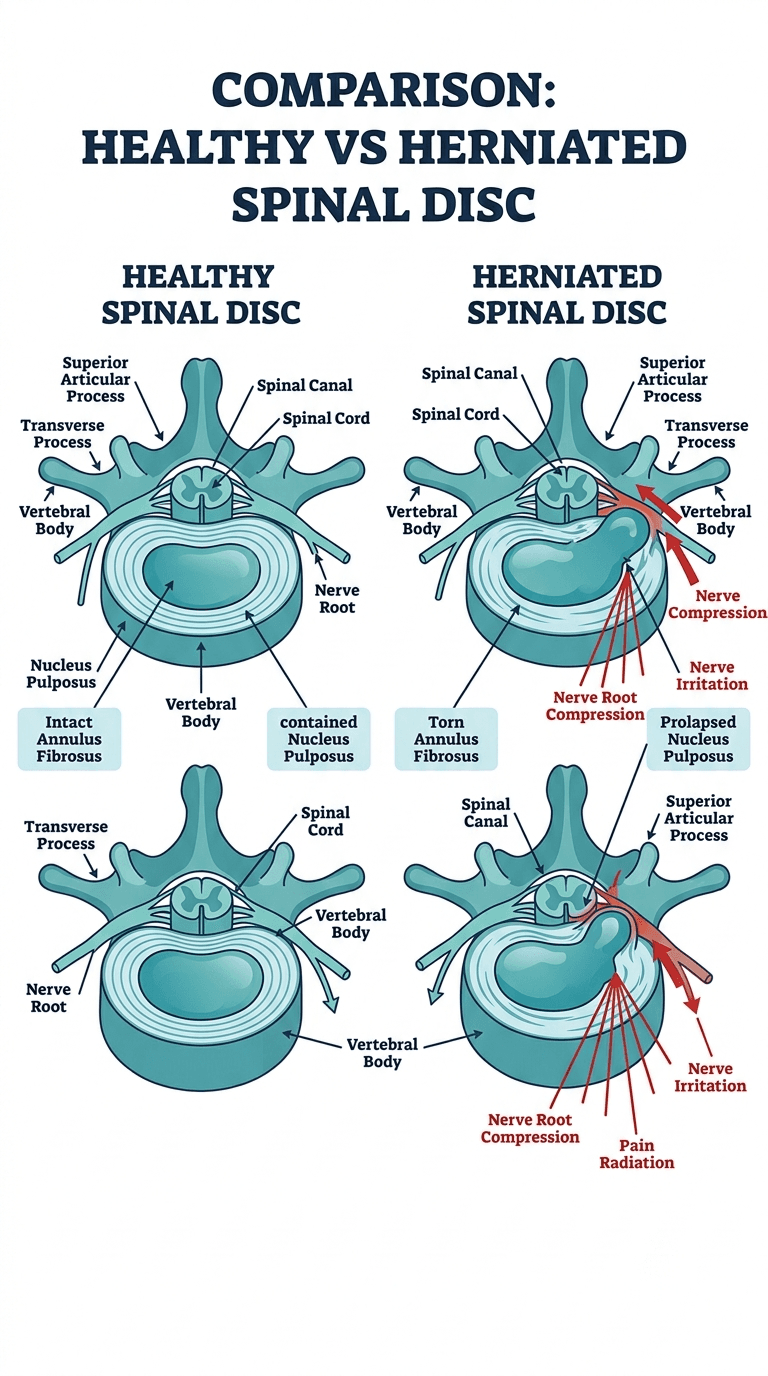
Your spine is a column of 24 vertebrae, each separated by a disc that acts as both a cushion and a hinge. Each disc has two parts: a tough outer ring called the annulus fibrosus and a gel-like center called the nucleus pulposus. A herniation happens when the nucleus pushes through a tear or weakness in the annulus. That alone may not cause symptoms. The problem comes when the displaced tissue presses against a nearby nerve root.
Most herniations happen in the lumbar spine (lower back), particularly at L4-L5 and L5-S1 - the two levels that carry the most mechanical load. Cervical herniations (in the neck) are less common but cause significant arm and hand symptoms when they do occur. Thoracic herniations in the mid-back are rare.
The disc doesn't have a great blood supply, which means it heals slowly and doesn't regenerate well. But the body has another trick: over time, the immune system recognizes the herniated material as foreign and begins to reabsorb it. This is part of why so many patients improve without intervention.
Who Gets Herniated Discs
Age 30 to 50 is the peak window. The discs have lost some of their water content by then (a normal aging process called desiccation), which makes the annulus more prone to tearing. Younger discs are actually more resilient; very old discs often herniate less dramatically because they've already stiffened.
Heavy lifting with poor form is the classic trigger, but many patients report no single moment of injury. Genetics play a larger role than most people expect - if a parent had significant disc disease, your risk is meaningfully higher. Prolonged sitting, especially in occupations requiring forward flexion, accelerates disc wear. Smoking impairs the nutrient supply to disc tissue and is an independent risk factor.
Recognizing the Symptoms
A herniated disc in the lower back typically causes sciatica: a shooting, burning, or electric pain that travels from the lower back through the buttock and down one leg, sometimes reaching the foot. The path of the pain maps to whichever nerve root is compressed. An L5 herniation tends to cause pain along the outer calf and into the big toe. S1 compression follows the back of the calf and into the heel and small toes.
Alongside the pain, many patients notice numbness or tingling in the same distribution. Muscle weakness - a heavy foot, difficulty pushing up onto one's toes, or weakness when flexing the big toe upward - indicates the nerve compression is more severe and warrants faster evaluation.
Neck herniations produce arm symptoms in a similar pattern: pain, tingling, or weakness radiating from the neck into the shoulder, arm, or hand, varying by which cervical level is involved.
One symptom that requires immediate emergency care is bowel or bladder dysfunction accompanied by saddle anesthesia (numbness in the groin and inner thighs). This can indicate cauda equina syndrome, a compression of the nerve bundle at the base of the spinal canal that constitutes a surgical emergency.
How It Gets Diagnosed
A clinical exam identifies the likely level of involvement in most cases. The straight-leg raise test is the most reliable physical maneuver - pain that reproduces below the knee when the examiner lifts a straight leg to 30-60 degrees strongly suggests nerve root compression.
MRI is the gold standard for imaging. It shows the disc, the spinal canal, and the nerve roots in detail. One important caveat: studies imaging asymptomatic adults find herniated discs in roughly 20-30% of people in their 30s and 40s, climbing to over 60% by age 60. That means an MRI finding has to match the clinical picture. A disc herniation that doesn't match your symptoms is not your problem.
CT scans and myelography are alternatives when MRI isn't possible. Plain X-rays show bone only - they don't visualize soft tissue and won't show a disc herniation directly.
Treatment: Starting Conservative
The standard starting point is a combination of time, activity modification, and targeted physical therapy. Complete bed rest is counterproductive; gentle movement maintains blood flow and prevents the muscle deconditioning that makes recovery harder.
Physical therapy focuses on core stabilization, posture correction, and specific directional movements that take pressure off the affected nerve. For many lumbar herniations, McKenzie exercises (extension-based movements) provide meaningful relief within a few weeks.
NSAIDs like ibuprofen or naproxen help manage inflammation and pain. Oral steroids - a Medrol dose pack or a short prednisone taper - are sometimes prescribed for acute flares. They don't treat the herniation itself but can break the cycle of severe pain long enough for the patient to engage in rehab.
Epidural steroid injections offer temporary relief for 40-50% of patients. They're most useful when pain is severe enough to prevent sleep or meaningful participation in physical therapy. They don't fix the disc, but they buy time and often turn out to be the only intervention needed. The relief typically lasts weeks to months, not years.
When Surgery Enters the Conversation
Surgery becomes the right discussion when three things are true: symptoms are severe or progressing, conservative treatment has failed after at least six weeks, and the imaging matches the clinical picture.
The most common surgical procedure for lumbar herniations is a microdiscectomy. The surgeon removes the fragment of disc that's pressing on the nerve through a small incision using a microscope. Recovery is faster than most patients expect - many go home the same day, and leg pain often improves dramatically within days. Back pain may take longer. The recurrence rate is 5-10%, meaning a small percentage herniate again at the same level.
Cervical herniations that fail conservative care are typically addressed with an anterior cervical discectomy and fusion (ACDF), where the disc is removed and the adjacent vertebrae are fused together. Cervical disc replacement is an alternative that preserves motion at the treated level, though not all patients are candidates.
Absolute surgical indications - situations where you don't wait six weeks - include progressive neurological weakness, cauda equina syndrome, or intractable pain that isn't responding to any conservative measure.
What Recovery Actually Looks Like
For patients treated conservatively, 50% improve meaningfully within one month, and 90% within three months. The first few weeks are often the hardest. Sciatica pain, in particular, can be severe even when the underlying process is resolving.
Post-surgery, microdiscectomy patients typically resume light activity within two to four weeks and return to physically demanding work in six to twelve weeks. Core strengthening and addressing the movement patterns that contributed to the herniation in the first place are non-negotiable parts of long-term management.
Recurrence is a real risk at the same or adjacent levels if the underlying biomechanics aren't addressed. That means weight management, core strength, ergonomic changes at work, and smoking cessation all matter.
If you've had leg or arm pain lasting more than two weeks, progressive weakness, or any bladder or bowel changes alongside spine symptoms, that's when to see an orthopaedic spine specialist. A single episode of back pain that comes and goes is manageable conservatively. Nerve symptoms that are worsening, or aren't improving after four to six weeks of appropriate treatment, deserve a proper evaluation.


