Tennis elbow, medically known as lateral epicondylitis, is frustratingly common. Despite its name, most people who get it have never held a tennis racket. It's an overuse injury that causes pain on the outside of the elbow, often radiating into the forearm. The pain can be sharp during certain movements or a dull constant ache that makes everyday tasks like gripping a coffee mug or turning a doorknob surprisingly difficult. Knowing what's actually happening in the tendon, and which treatments have real evidence behind them, can save a lot of wasted time and money.
The anatomy of annoyance
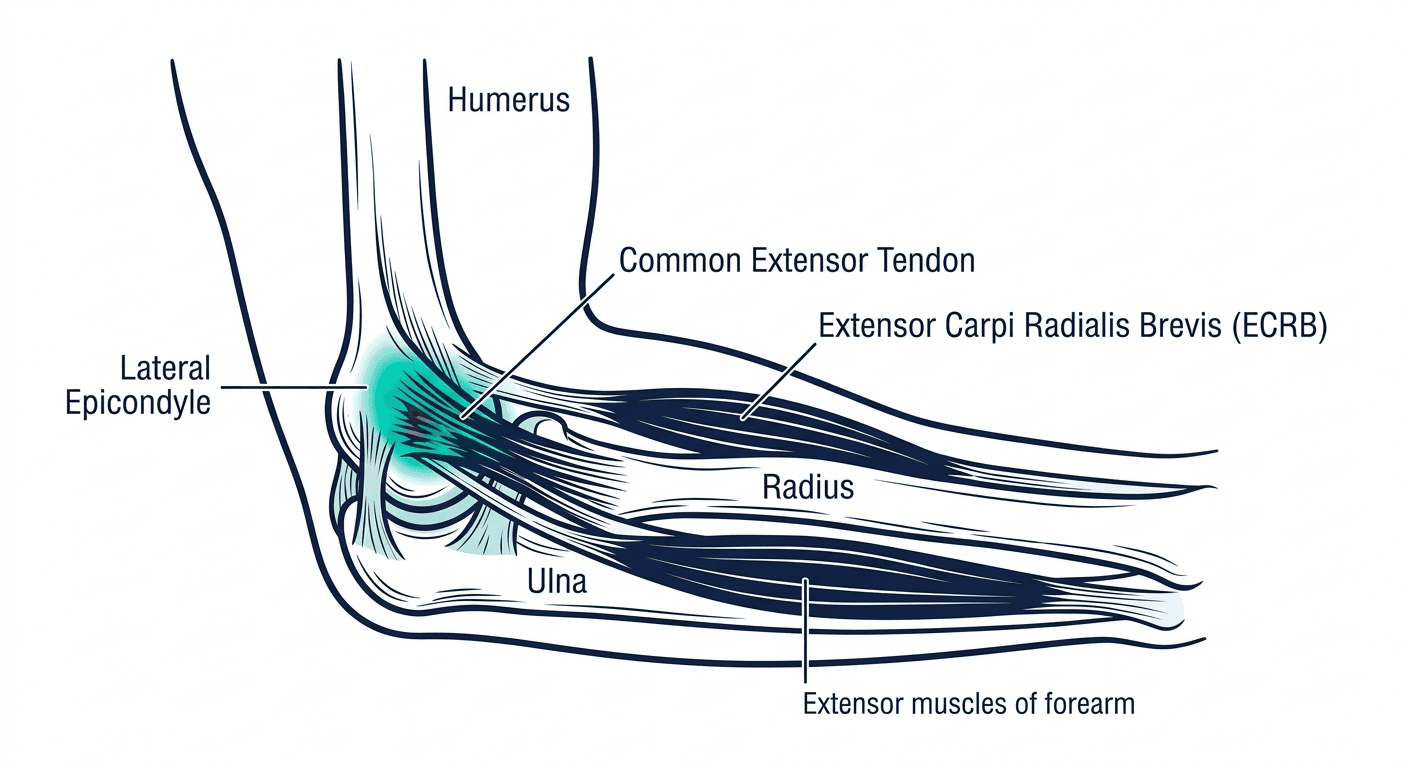
The lateral epicondyle is a bony bump on the outside of the humerus, just above the elbow joint, where several wrist-extending muscles attach. This collective attachment is called the common extensor origin. The main culprit in tennis elbow is almost always the extensor carpi radialis brevis (ECRB) tendon.
The ECRB helps extend and abduct the wrist. Repeated gripping and twisting puts steady stress on its attachment point - a constant tug at the same small patch of bone.
Why your elbow hates you
Tennis elbow isn't primarily an inflammatory condition, despite the "-itis" suffix. It's degenerative. We used to call it tendonitis, implying acute inflammation, but that framing isn't quite right. What actually happens is that repetitive microtrauma breaks down the collagen fibers in the ECRB. The body tries to repair the damage but produces disorganized, immature tissue instead of strong organized collagen. This pathological change, called angiofibroblastic hyperplasia, leaves the tendon structurally weaker and persistently painful.
Any activity involving repetitive gripping, wrist extension, or forearm rotation drives the process. Screwdrivers, hammers, extended typing, lifting palm-down - it accumulates.
Who actually gets this
Tennis elbow affects about 1-3% of adults annually, most commonly between ages 30 and 50. Only about 5-10% of those diagnosed actually play tennis. For them, it's usually technique, grip size, or string tension.
Everyone else: carpenters, plumbers, painters, mechanics, cooks, office workers, musicians. Jobs and hobbies that repeat the same hand-and-wrist motion thousands of times. The demands on the tendon outpace its ability to recover.
Diagnosis
Diagnosing tennis elbow doesn't require imaging. A physical exam is usually enough.
The doctor will press on the lateral epicondyle and ECRB tendon origin, looking for the tenderness that's the most consistent finding. A few provocative tests help confirm it. Cozen's test: you make a fist, pronate your forearm (palm down), and extend your wrist against resistance - pain on the outside of the elbow is positive. Maudsley's test resists extension of the middle finger. Mill's test passively stretches the extensor tendons by flexing the wrist, pronating the forearm, and extending the elbow at the same time.
X-rays won't show the tendon but can rule out arthritis, bone spurs, or stress fractures. Ultrasound or MRI is useful for stubborn or diagnostically unclear cases - both can show tendon thickening, degeneration, or partial tears - but they're rarely the first step.
What actually works
About 80-95% of tennis elbow cases resolve without surgery. The downside: it takes time, and the people who get impatient around week four tend to end up with chronic cases.
Initial management
Activity modification doesn't mean stopping everything - complete rest often makes things worse. It means identifying which specific movements aggravate symptoms and adjusting them. Ice for 15-20 minutes after activity helps with pain. NSAIDs like ibuprofen or naproxen manage symptoms but don't fix the underlying tendon problem.
Physical therapy
Physical therapy is where most of the actual recovery happens. The most evidence-backed approach is eccentric loading: exercises where the tendon is lengthened under tension, which gradually stimulates collagen production and remodels tendon structure.
The standard wrist extensor protocol is simple. Sit with your forearm resting on a table, wrist hanging off the edge palm-down, holding a light dumbbell (start with 1-2 lbs). Slowly lower the weight, letting your wrist flex toward the floor. Use your other hand to return to the starting position. Three sets of 15, twice a day. The slow controlled lowering is the point - not the lift back up.
A full PT program will also include wrist extensor and flexor stretching, manual therapy to address scar tissue (techniques like IASTM), progressive forearm and grip strengthening once pain allows, and an ergonomic assessment of whatever's creating the repetitive load in the first place.
Bracing helps with day-to-day symptoms. A counterforce strap worn just below the elbow compresses the forearm muscles and shifts load away from the epicondyle - many people get noticeable relief during activity, though it doesn't fix the tendon. A wrist splint worn at night keeps the extensor tendons in a rested position.
Recovery timelines
Significant improvement takes 6 weeks to 6 months, depending on severity and how consistently you follow the program. Progress isn't linear. Most people see some relief, hit a plateau around weeks 3-4, and give up. That plateau isn't a sign that things aren't working - it's normal tendon remodeling pace.
The cortisone problem
Cortisone injections were the standard treatment for decades. A shot can dramatically reduce pain within days, which feels like real progress. The longer-term data is less encouraging.
Multiple studies comparing cortisone to physical therapy show cortisone patients often have worse outcomes at 6 and 12 months - higher recurrence rates and, in some cases, structurally weaker tendons. The mechanism isn't surprising: cortisone is anti-inflammatory, but tennis elbow isn't primarily an inflammatory process. It suppresses symptoms while potentially interfering with whatever repair the tendon is attempting. Repeated injections make this worse.
Cortisone has a narrow role: breaking a severe pain cycle quickly enough to allow someone to actually start physical therapy. As a standalone treatment, the evidence doesn't support it.
PRP: promise vs. reality
Platelet-rich plasma (PRP) involves drawing your blood, spinning it to concentrate platelets and growth factors, then injecting that solution directly into the damaged tendon. The idea is to flood the site with healing proteins and restart a repair process the tendon has failed to complete on its own.
The evidence is mixed. Some trials show PRP outperforms cortisone at 6 and 12-month follow-ups, with lower recurrence. Others find it no better than a solid PT program. No study has convincingly shown it beats good physical therapy. Cost runs $500-$2,000 per injection, almost never covered by insurance. Expect a pain flare for a few days after the injection, then slow improvement over weeks to months.
It's a reasonable option for cases that haven't responded to 4-6 months of proper conservative care. It works best alongside ongoing PT, not instead of it.
When all else fails: surgery
Surgery is for people who still have significant pain after 6-12 months of genuine conservative treatment - PT done consistently, activity modified, bracing tried. If pain is limiting work or basic daily function after that timeline, surgery is worth discussing.
The procedure removes the degenerated tendon tissue and stimulates fresh healing. Most surgeons use an open release: a 1-2 inch incision over the lateral epicondyle, damaged ECRB tissue removed, sometimes with a partial release from the bone. Arthroscopic surgery uses smaller incisions and a camera; percutaneous release uses a needle through a small puncture. All three have similar success rates - around 80-90%.
Recovery still takes months: a splint for 1-2 weeks, range-of-motion work beginning shortly after, strengthening around 6-8 weeks out, and full return to heavy activity at 3-6 months, sometimes longer.
The stubborn case
Six months of proper conservative treatment with little improvement warrants a harder look before escalating to surgery.
Compliance is the most common issue. Doing exercises sporadically, or continuing the activity that's causing the problem, stalls recovery entirely. But it's also worth questioning the diagnosis. Radial tunnel syndrome (nerve compression near the elbow), cervical radiculopathy (a nerve pinch in the neck), and posterolateral rotatory instability of the elbow can all cause lateral elbow pain and get treated as tennis elbow for months without improving. If you're not getting better, the diagnosis might be wrong.
Underlying medical conditions matter too. Poorly controlled diabetes, thyroid dysfunction, and certain medications all impair tendon healing. Shoulder weakness or persistent ergonomic problems keep the tendon under load it can't handle. Chronic pain also changes how pain is processed centrally, and psychological stress genuinely slows musculoskeletal recovery - not as a character flaw, just as physiology.
Numbness or tingling in the hand, or pain that wakes you from sleep, should prompt a specialist visit rather than continued self-management. An orthopedic surgeon can confirm the diagnosis, rule out nerve involvement, and lay out the realistic options - including whether surgery actually makes sense for your specific case.


