Broström Procedure
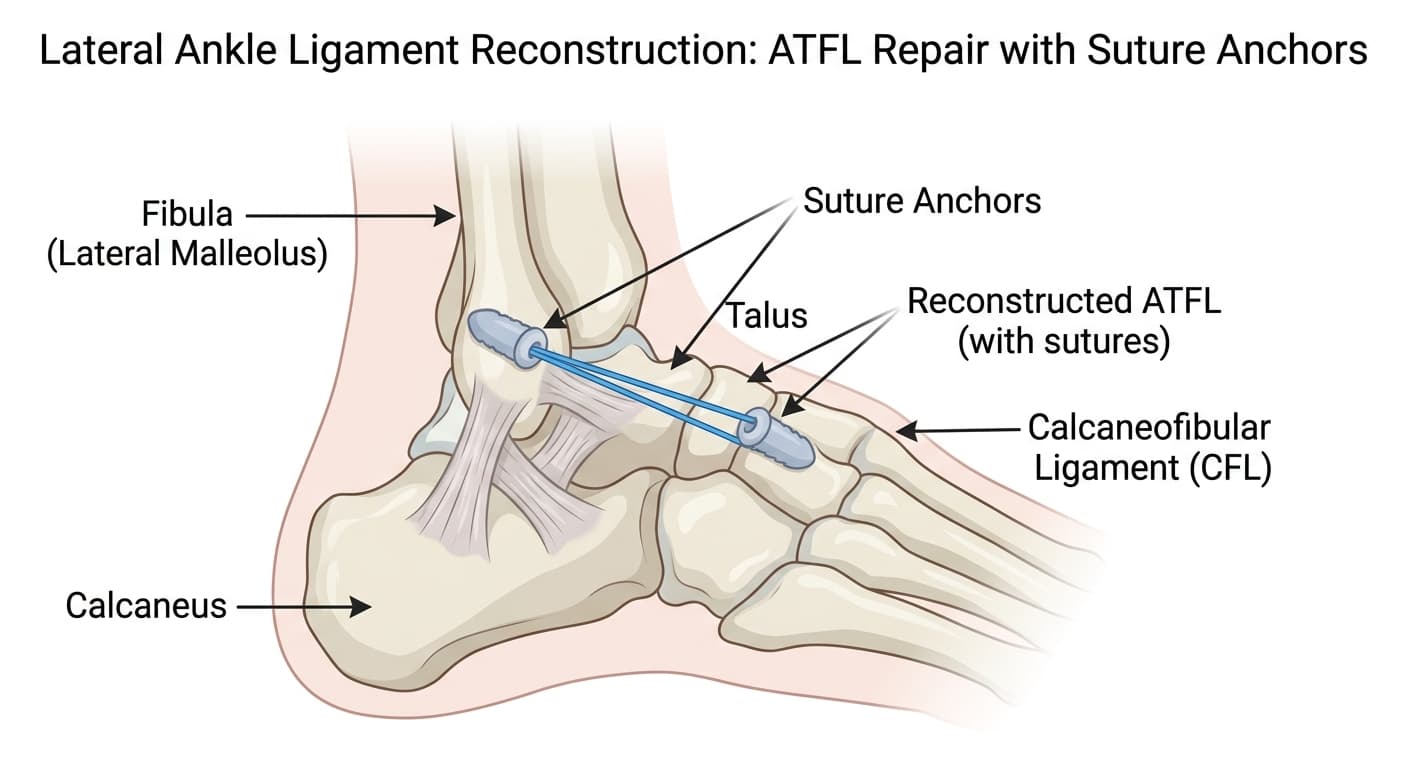
The Broström procedure is the standard surgical reconstruction for chronic lateral ankle instability. After ankle sprains that haven't healed properly, the anterior talofibular ligament (ATFL) and often the calcaneofibular ligament (CFL) remain stretched and lax, causing the ankle to give way repeatedly during activity. The surgeon directly repairs these ligaments by shortening and reattaching them to the fibula, restoring their tension. A modification (Gould modification) reinforces the repair with a flap of the inferior extensor retinaculum. The procedure produces lasting stability in 85-90% of patients at long-term follow-up.
Find a SurgeonWhat is Broström Procedure?
The Broström procedure is the standard surgical reconstruction for chronic lateral ankle instability. After ankle sprains that haven't healed properly, the anterior talofibular ligament (ATFL) and often the calcaneofibular ligament (CFL) remain stretched and lax, causing the ankle to give way repeatedly during activity. The surgeon directly repairs these ligaments by shortening and reattaching them to the fibula, restoring their tension. A modification (Gould modification) reinforces the repair with a flap of the inferior extensor retinaculum. The procedure produces lasting stability in 85-90% of patients at long-term follow-up.
Typical cost: $8,000 - $18,000. Cost increases if combined with ankle arthroscopy. Covered by most insurance when chronic instability is documented and conservative treatment has failed. Athletes seeking to return to high-level sport are strong candidates for surgical approval.
Last reviewed June 14, 2026 by AdvOrtho Editorial Team
Informational, not medical advice
Who Needs Broström Procedure?
Patients with documented chronic lateral ankle instability - defined as recurrent giving-way episodes or persistent functional instability over at least 6 months despite a structured rehabilitation program focused on peroneal strengthening and proprioceptive training. Stress X-rays or MRI typically confirm ligament laxity before surgical planning. Active patients, athletes, and those whose instability limits daily activities or sport are the typical candidates.
What to Expect
Recovery Timeline
Non-weight-bearing in a cast or boot. Leg elevation to minimize swelling. Sutures removed at 10-14 days.
Protected weight-bearing in a boot begins around weeks 2-3 when pain allows. Range-of-motion exercises initiated.
Transition from boot to lace-up ankle brace. Physical therapy: peroneal strengthening, proprioception training, single-leg balance.
Return to running in a straight line. Sport-specific agility and cutting drills begin.
Return to full sport with a functional brace for contact sport or high-risk activities. Most athletes return to competition by month 5-6.
Risks & Complications
- Sural nerve injury - the nerve runs near the incision and can cause numbness along the outer foot
- Stiffness or restricted inversion (the repair tightens the ankle; over-tightening limits inversion range)
- Re-injury and failure of the repair if return-to-sport is rushed
- Wound healing issues
- Continued instability requiring revision with a tendon graft (allograft or autograft augmentation)
- Ankle arthritis acceleration if pre-existing cartilage damage was not addressed at the time of surgery
Frequently Asked Questions
Does the Broström procedure work for everyone with chronic ankle instability?
The Broström procedure works best when the ligaments are stretched but the tissue quality is adequate for direct repair. In patients who have had multiple prior ankle surgeries, in those with generalized ligamentous laxity (hypermobility), or when the ligament tissue has degenerated too much to repair directly, surgeons augment the Broström with a tendon graft (typically from the peroneus brevis or an allograft). The decision is made intra-operatively or pre-operatively based on MRI findings. Pure direct Broström repairs have a 10-15% long-term failure rate; augmented repairs are more durable in high-risk patients.
Do I need ankle arthroscopy along with the Broström?
Many surgeons perform arthroscopy first as a routine part of the procedure, since osteochondral lesions (cartilage injuries on the talus) are found in 40-65% of patients with chronic ankle instability who have imaging. If an unaddressed cartilage lesion is left untreated, it continues to cause symptoms after the instability is corrected. Arthroscopy adds 20-30 minutes to the procedure and increases cost slightly, but addressing both problems in one surgery is generally preferred over returning for a second operation.
What happens if I sprain the ankle again after the Broström?
A re-sprain after a successful Broström is possible. The repaired ligaments are mechanical structures - they can be re-torn with significant force. Most patients are counseled to use a lace-up brace for high-risk activities (trail running, court sports, skiing) indefinitely, not because the surgical result is weak, but because no ligament - native or repaired - is indestructible. A significant re-sprain after surgery warrants MRI and repeat evaluation. In some cases the repair holds and the symptoms resolve with rehabilitation; in others, revision surgery with tendon augmentation becomes necessary.
Find a surgeon for Broström Procedure
Compare orthopedic surgeons who perform this procedure.
Search surgeonsEstimated Cost
$8,000 - $18,000. Cost increases if combined with ankle arthroscopy. Covered by most insurance when chronic instability is documented and conservative treatment has failed. Athletes seeking to return to high-level sport are strong candidates for surgical approval.
Related Specialty
Foot & Ankle Specialists →Related Conditions
Other Procedures
From the Resource Center
This information is for educational purposes only. Costs are estimates and vary by location, surgeon, and insurance. Always consult a qualified healthcare provider.