MPFL Reconstruction
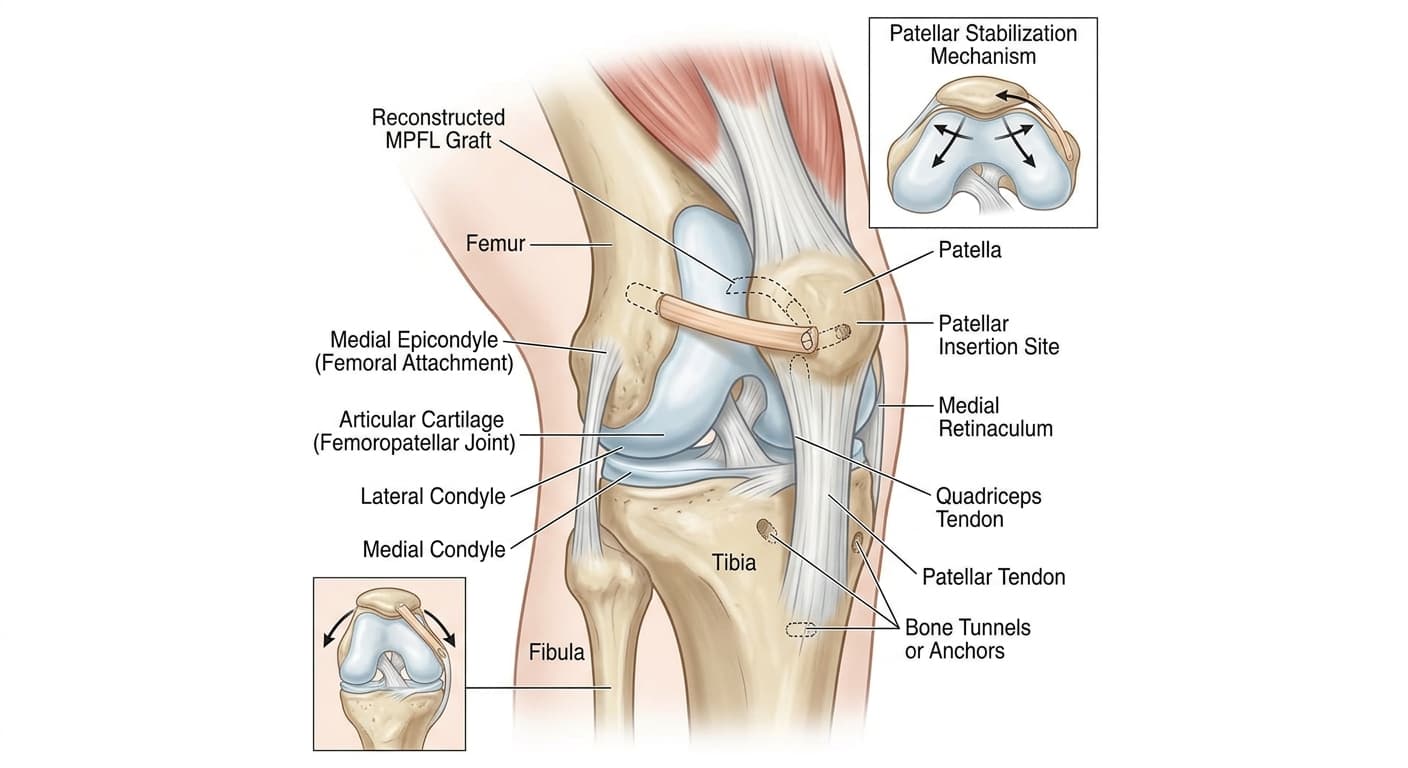
MPFL reconstruction (medial patellofemoral ligament reconstruction) restores the primary soft-tissue restraint that prevents the kneecap from dislocating outward. The MPFL runs from the inner side of the kneecap to the femur and is torn in virtually every acute patellar dislocation. When the ligament fails to heal correctly after one or more dislocations, the kneecap remains prone to giving way. The surgeon reconstructs the MPFL using a tendon graft - typically the gracilis or semitendinosus from the same knee, or occasionally an allograft - fixed to the patella and femur with suture anchors or an interference screw. The procedure is often combined with tibial tubercle osteotomy (TTO) when the tibial tubercle is significantly lateralized.
Find a SurgeonWhat is MPFL Reconstruction?
MPFL reconstruction (medial patellofemoral ligament reconstruction) restores the primary soft-tissue restraint that prevents the kneecap from dislocating outward. The MPFL runs from the inner side of the kneecap to the femur and is torn in virtually every acute patellar dislocation. When the ligament fails to heal correctly after one or more dislocations, the kneecap remains prone to giving way. The surgeon reconstructs the MPFL using a tendon graft - typically the gracilis or semitendinosus from the same knee, or occasionally an allograft - fixed to the patella and femur with suture anchors or an interference screw. The procedure is often combined with tibial tubercle osteotomy (TTO) when the tibial tubercle is significantly lateralized.
Typical cost: $12,000 - $25,000 for isolated MPFL reconstruction. Cost increases by $5,000-$10,000 when combined with tibial tubercle osteotomy. Covered by most insurance for patients with recurrent dislocations. First-time dislocation coverage varies by plan - documentation of risk factors (trochlear dysplasia, TT-TG measurement) strengthens the case.
Last reviewed June 15, 2026 by AdvOrtho Editorial Team
Informational, not medical advice
Who Needs MPFL Reconstruction?
Patients who have dislocated their kneecap more than once, or those with a first-time dislocation and significant risk factors for recurrence: age under 25, trochlear dysplasia (shallow groove), patella alta (high-riding kneecap), or a high TT-TG distance on imaging. Recurrence after a first dislocation is 15-50% without surgery; after a second dislocation, the rate without surgical stabilization climbs higher. Patients who experience the kneecap "sliding" or giving way during activity without full dislocation are also candidates.
What to Expect
Recovery Timeline
Brace locked in extension, crutches. Quadriceps activation exercises begin immediately. Straight-leg raises. Ice and elevation.
Brace unlocked for walking. Begin cycling on a stationary bike. Closed-chain strengthening (mini squats, leg press).
Progressive strengthening, balance, and proprioception training. Running begins around month 4 when strength criteria are met.
Sport-specific agility and cutting drills. Return to non-contact sport for most patients by month 5-6.
Return to full contact sport. TTO cases may need an additional month. Strength symmetry testing before clearance.
Risks & Complications
- Patellar fracture if the bone tunnels weaken the patella
- Graft over-tightening causing medial patellar pain or limited flexion
- Recurrent dislocation if graft stretches or fixation fails
- Donor site pain at the hamstring harvest site
- TTO non-union if combined (uncommon)
- Stiffness - the most common complaint in the early recovery phase
- Cartilage damage acceleration if pre-existing lesions are present
Frequently Asked Questions
Do I need surgery after a first-time patellar dislocation?
Not always, but it depends on your anatomy. For most first-time dislocators, a structured rehabilitation program focused on quadriceps and hip strength reduces but does not eliminate re-dislocation risk. However, imaging findings matter significantly: if CT or MRI shows trochlear dysplasia (a flat or convex femoral groove), patella alta (high-riding kneecap), or a TT-TG distance greater than 20 mm, the mechanical setup of your knee makes the kneecap prone to re-dislocation regardless of how well you rehabilitate. Young patients with these anatomical risk factors who depend on their knees for sport often choose early surgery over waiting for a second dislocation.
What is the TT-TG distance and why does it matter?
The TT-TG (tibial tubercle to trochlear groove) distance measures how far laterally the tibial tubercle - the bony bump below the kneecap where the patellar tendon attaches - sits relative to the center of the femoral groove. A higher number means the kneecap is being pulled more strongly toward the outside of the knee throughout the range of motion. When TT-TG exceeds 20 mm, a tibial tubercle osteotomy (moving the attachment point medially) is typically added to MPFL reconstruction to address the mechanical malalignment, not just the torn ligament.
Will my kneecap ever feel normal again after reconstruction?
Most patients report that the instability feeling - the sense that the knee could give way - resolves completely after successful MPFL reconstruction. Cartilage damage from prior dislocations can cause ongoing aching that surgery does not fix; that is a separate problem from instability. Return to sport rates are high (over 80% in most studies), though some patients describe a persistent mild awareness of the reconstructed knee that is not painful but noticeable. Full functional recovery takes 6-9 months, and the knee often continues to improve subtly through the first year.
Find a surgeon for MPFL Reconstruction
Compare orthopedic surgeons who perform this procedure.
Search surgeonsEstimated Cost
$12,000 - $25,000 for isolated MPFL reconstruction. Cost increases by $5,000-$10,000 when combined with tibial tubercle osteotomy. Covered by most insurance for patients with recurrent dislocations. First-time dislocation coverage varies by plan - documentation of risk factors (trochlear dysplasia, TT-TG measurement) strengthens the case.
Related Specialty
Sports Med Specialists →Related Conditions
Other Procedures
From the Resource Center
This information is for educational purposes only. Costs are estimates and vary by location, surgeon, and insurance. Always consult a qualified healthcare provider.